Interventions to Prevent Fall – Research Results
Data Analysis and Findings
Part 1 – Demographic Profile
Table1. Age Distribution
|
Age Range |
F |
% |
|
26-30 |
3 |
30 |
|
31-35 |
3 |
30 |
|
36-40 |
1 |
10 |
|
41-45 |
0 |
0 |
|
46-50 |
2 |
20 |
|
51-55 |
1 |
10 |
|
Total |
n = 10 |
n = 100 |
Graph
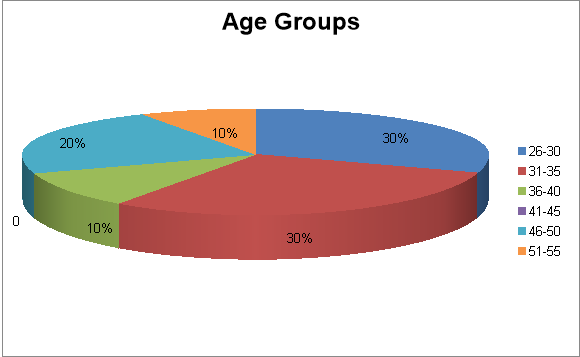
Interpretation
Majority of the respondents were between 26-30 and 31-35 age groups. 20% respondents were of 46-50 years of age and 10% respondents were of 36-40 and rest 10% belongs to 51-55 years of age.
Table 2. Sex
|
Sex |
F |
% |
|
Female |
10 |
100 |
|
Male |
0 |
0 |
|
Total |
n = 10 |
n = 100 |
Graph
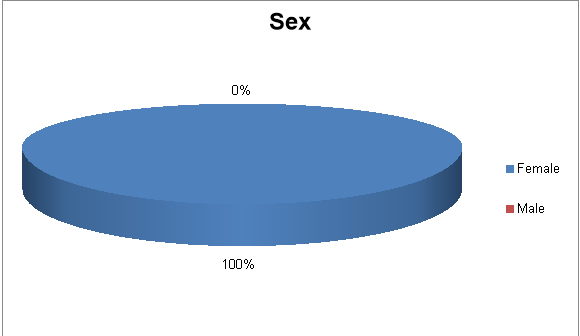
Interpretation
All the participants (healthcare assistants) were female working at CHT Royal Oak Rest Home.
Table.3 Ethnicity
|
Ethnicity |
F |
% |
|
Indian |
7 |
70 |
|
Fijian |
1 |
10 |
|
Japanese |
1 |
10 |
|
Kiwi |
1 |
10 |
|
Total |
n = 10 |
n = 100 |
Graph
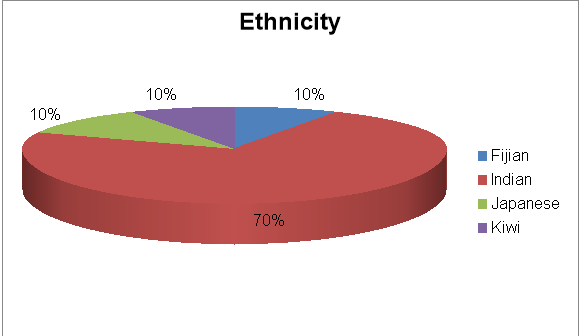
Interpretation
Majority of the participants were Indian (70%). Rest 30% of the participants were Fijian, Japanese and Kiwi respectively.
Table 3. Work Status
|
Work Status |
F |
% |
|
Permanent Full time |
7 |
70 |
|
Permanent Part time |
1 |
10 |
|
Casual Part time |
2 |
20 |
|
Total |
n = 10 |
n = 100 |
Graph
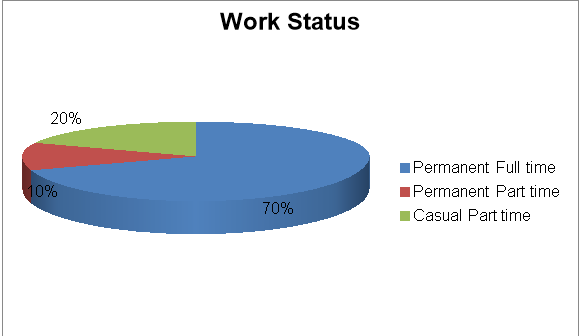
Interpretation
70% of the participants (Healthcare Assistants) were permanent full time employees whereas 20% of the participants were casual part time and 10% participants were permanent part time employees.
Part II. Data Analysis and findings
This research finding indicated that the best practices for fall prevention used by Healthcare Assistants were use of aids such as wheelchair and stick (50%), hazard identification (40%), signs for wet floor (30%), care plans and monitoring (30%), clutter free environment (30%), bell ring (10%) and sensor mat (10%).
The immediate interventions used by healthcare assistants if they encountered fall incidence were injury risk assessment (50%), fill the ACC incident form (50%), ask help from others (50%), first aid (40%), inform nurse (40%), call ambulance (30%), give reassurance to the residents (20%) and use hoist (20%).
This research indicated that CHT Royal Oak rest home provides ongoing training to all the staff of the organisation about moving and handling the residents.
Furthermore, the fall incidence was being reported and documented by healthcare assistants by filling ACC incidence/Accident forms (100%), informing manager, Register Nurse and family (50%) and using progress notes (20%).
Implication
The use of best practices to prevent fall at rest home engaged the healthcare assistants to increase confidence, knowledge, skills and abilities in the identification of residents within health care facilities at risk of falling and to define interventions for the prevention of falling in order to achieve the vision of the organisation.
Recommendation
Although, CHT Royal Oak is competent enough to practice best interventions to prevent fall, there is always room for continuous improvement. It is hereby recommended that manager should assess and document all resident for intrinsic risk factors to fall such as history of a recent fall, specific co-morbidities: dementia, hip fracture, type 2 diabetes, Parkinson’s disease, arthritis, and depression and any functional disability or use of assistive device. Furthermore, patient care environment should also be assessed routinely for extrinsic risk factors to fall such as floor surfaces for spills, wet areas, unevenness, proper level of illumination and functioning of lights (night light works), table tops, furniture, beds should be sturdy and are in good repair and if needed, institute corrective actions. It is recommended to use standardized environmental checklists to document findings and re-evaluate environment for safety.
Moreover, the healthcare staff should promote early mobility and incorporate measures to increase mobility, such as daily walking, balance training, strengthening and weight bearing exercise, if medically stable and not otherwise contraindicated. General safety precaution and fall prevention strategies such as medication review; use of proper footwear, proper continence management should be implemented. Multidisciplinary plan of care for prevention and follow up monitoring should be done to prevent falls in healthcare organisation.
In addition to that, education regarding procedures to follow in the event of a fall should be provided to the staff as well as to the residents. The goal of education among residents is to increase the awareness of falls risks and preventative strategies, thus decreasing the number and severity of falls. Education may improve the resident’s self-confidence therefore reducing the fear of falling.The most up to date information needs to be available and provided in order to educate residents effectively. All staff should be involved in this process, as each one is an important member of the health care team. Lastly, health care workers should be given training to increase their awareness of residents who are at risk of falling by giving them staff education brochure for fall, through visual aids and posters etc.
Conclusion
This study involved the healthcare assistants of CHT Royal Oak Ret Home to know the best practices among them to prevent fall in this facility. To sum up, the healthcare assistant showed quite good knowledge and awareness regarding best interventions they are using for fall prevention. Regular ongoing training for fall prevention was provided to all the staffs of CHT Royal Oak Home. Furthermore, fall prevention practices constitute the basics of patient safety. They apply across all rest home areas and help safeguard not only residents, but also visitors and staff in many cases. By this way, this research helps to improve and to better understand the best interventions that are used by healthcare staff and to implement the best policy to prevent fall worldwide.
References
CHT. (2015). About us. Retrieved from http://www.cht.co.nz/about-us-2/
Creswell, J. W. (2003). Research design: Qualitative, quantitative, and mixed method approaches. Thousand Oaks, CA: Sage Publications. Retrieved from http://isites.harvard.edu/fs/docs/icb.topic1334586.files/2003_Creswell_A%20F ramework%20for%20Design.pdf
Gama, Z. A., Medina-Mirapeix, F., & Saturno, P. J. (2011). Ensuring Evidence-Based Practices for Falls Prevention in a Nursing Home Setting. Journal of the American Medical Directors Association, 12(6), 398-402. doi:10.1016/j.jamda.2011.01.008
Health Quality & Safety Commission New Zealand. (2014). Falls in older people: the impacts. Retrieved from http://www.hqsc.govt.nz/assets/Falls/10- Topics/topic1-falls-in-older-people-15-April-2014.pdf
Ministry of Health. (2016). What is an interventions. Retrieved from health.mo.gov/data/interventionmica/index_4.html
Nass, S. J., Levit, L. A., Gostin, L. O., & Institute of Medicine (U.S.). (2009). Beyond the HIPAA privacy rule: Enhancing privacy, improving health through research. Washington, DC: National Academies Press.
Phelan, E. A., Aerts, S., Dowler, D., Eckstrom, E., & Casey, C. M. (2016). Adoption of Evidence-Based Fall Prevention Practices in Primary Care for Older Adults with a History of Falls. Frontiers in Public Health, 4. doi:10.3389/fpubh.2016.00190
Shever, L. L., Titler, M. G., Mackin, M. L., & Kueny, A. (2010). Fall Prevention Practices in Adult Medical-Surgical Nursing Units Described by Nurse Managers. Western Journal of Nursing Research, 33(3), 385-397. doi:10.1177/0193945910379217
World Health Organisation. (2016). Falls. Retrieved from http://www.who.int/mediacentre/factsheets/fs344/en/