Rohingya Refugees Health Problems and Health Seeking
Title: HEALTH PROBLEMS & HEALTH CARE SEEKING BEHAVIOR OF ROHINGYA REFUGEES
Abstract
Background.Rohingya refugees are the most vulnerable group due to lack of health care system, personal hygiene, shelter, sanitation and violence. In this study the main aim to find out the health problems & health care seeking behavior of rohingya refugee peoples, to identify the socio-demographic information for such exposure group in relation to age, sex, occupation, living areas, to explore the patient’s physical, emotional, perceptions, attitudes and environmental health problems and to bring out health care seeking behavior of refugees. Methodology: This was a cross-sectional study. Total 149 samples were selected conveniently for this study from the refugee camps. Data was collected by using mixed type of questionnaire. Descriptive statistic was used for data analysis which focused through table, pie chart and bar chart. Results: The finding of the study showed that 45.6% participants had multiple problems followed by 16.8% participants had other specific problems like musculoskeletal pain, visual problems and peptic ulcer. Urinary tract infection is the leading individual health problems, among the participants 11.4% had this problem, 10.7% participants had hypertension, 6% had respiratory tract infection, 3.4% had nutrition deficiency, 4.75% had diabetes mellitus and 1.3% had sanitation & hygiene problems. Among the participants the middle age people had mostly health problems, 68.4% age range between 15-59 years. The study showed that, only 16.1% participants were satisfied with the quality of service they received, among the participants 37.6% participants said that they were need better services such as more laboratory test, radiological imaging, more medicine & more doctors. Conclusion:It is clear that refugee peoples suffered from lots of health problems, because there living condition, environmental situation not similar like an independent nations, from being their expectation there was not sufficient enough medicine & other services were available, they deserve better services.
Keywords:Health problems, Rohingya refugee, Health seeking behaviour, Bangladesh.
Introduction:
Rohingyas are an ethnic, linguistic and religious minority group of Northern Rakhine State (NRS) of Myanmar. Myanmar government categorized them as illegal immigrants from Bangladesh and excluded them from citizenship and basic human rights (1). From 1991-1992 a mass exodus of more than 250,000 Rohingya refugees fled persecution in the Union of Myanmar and arrived in Bangladesh, living in temporary camps and completely dependent on outside support from the United Nations (UN), the Government of Bangladesh (GOB) and numerous non-governmental organizations (NGOs) (2,3,4). Globally, the total population of refugees is about 9.9 million. The general health status of refugees in various countries is reported to be poor with malnutrition being the major health problem due to lack of access to sufficient food and nutrient intakes. Other health problems among refugees include mental illnesses, intestinal parasites, hepatitis B, tuberculosis, sexually transmitted diseases, HIV/ AIDS, malaria and anemia (2, 5). Infants and young children are often the earliest and most frequent victims of violence, disease, and malnutrition which accompany population displacement and refugee outflows. Rohingyas are spending long period of time in Bangladesh as refugees “My life is over. All I want is for my children to have a chance at a better life.” Two generations of the Rohingya have said this. The vast majority of their community suffers the same neglect and lack of opportunity that their parents faced at present, there are no specific services available to refugee children with special needs or disabilities. With regards to cases of sexual exploitation of children, there have been reports and cases of refugee minors (females) being harassed, abused or raped by local villagers. A survey found that out of 508 children of under 5 years of age, 65% were anemic and therefore, chronically malnourished (4, 6, 7). Rohingya is a generic term referring to the Sunni Muslim inhabitants of Arakan, the historical name of a Myanmar border region which has a long history of isolation from the rest of the country. It is thought that the Rohingya are of mixed ancestry, tracing their origins both to outsiders (Arabs, Moors, Turks, Persians, Moguls and Pathans) and to local Bengali and Rakhine. They speak a version of Chittagonian, a regional dialect of Bengali which is also used extensively throughout south-eastern Bangladesh (8). Syrian refugees are in need of basic services such as shelter, nutrition, education, medication and health care services. Approximately 1.4 million Syrian refugees are children and the United Nations Children’s Fund has reported that these children are at risk of being a “lost generation.” Syrian refugees are enduring daily challenges to physical and mental survival. In addition to the extreme needs for physical and nutritional interventions, mental health professionals recognize the urgent need for counseling services based on widespread documented reports of refugees (9, 10). Three meals a day are served in camps, but refugees are not satisfied with the quality of what is served. There are occasional cases of food intoxication. Refugees are not allowed to cook their food in tents because of the risk of fire. Out of camps, the nutritional status of refugees is mostly bad, only limited number of them can have 3 meals a day. In general, they feed on bread and vegetables. A survey conducted at a provincial centre found, among women in the age group 15-49, iron (by 50%) and B12 vitamin deficiency (by 46%) (11). Some of the countries in the region (notably Pakistan, Bangladesh, and Nepal) are host to refugee and displaced populations from neighbouring states, a circumstance that in itself merits attention since it has the potential to cause major political unrest (12). Bangladesh is surrounded by a high HIV prevalence neighboring country at southern part, Myanmar. Teknaf is a small town in the Chittagong Division at the southern tip of Bangladesh, separated from Myanmar on the eastern side by the river Naf. This border area is unique for many reasons, including the history of the tens of thousands of refugees that are currently living in squalid conditions on the Bangladeshi side (13). A 19 years old refugee at Nayapara camp sayed that “I was born in Burma, but the Burmese government says I don’t belong there. I grew up in Bangladesh, but the Bangladesh government says I cannot stay here. As a Rohingya, I feel I am caught between a crocodile and a snake” (14). The population of Bangladesh is growing at approximately the rate of l.59 percent per annum the percentage of urban population is 27% while that of rural is 73%. Bangladesh’s population growth rate was among the highest in the world in the 1960s and 1970s, when the country swelled from 65 to 110 million (15).
The Rohingya refugee problem has been a longstanding issue and involves the question of an ethnic minority’s identity. The Rohingyas are an ethnic minority group in the northern Arakan (currently Rakhine) state of Myanmar. Commonly known as Muslim Arakanese, the Rohingyas trace their historical roots in the Arakan region from the eleventh century to 1962 (16). Hundreds more Rohingya have been the victims of torture, arbitrary detention, rape, and other forms of serious physical and mental harm. Whether confined to the three townships in northern Rakhine State or to one of dozens of internally displaced persons camps throughout the state, Rohingya have been deprived of freedom of movement and access to food, clean drinking water, sanitation, medical care, work opportunities, and education (17). There is no domestic law in Bangladesh to regulate the administration of refugee affairs or to guarantee refugee rights. New refugees have difficulties accessing health care, their health problems may worsen with time.5 Social isolation and disconnection have been shown to contribute to premature death among members of isolated communities (18).
In refugee camps medical services are mostly crippled, there is no examination and with the exception of some community health centers (RHU) there is no pregnant women and infant monitoring either, since family planning services for refugees are not available, there are unwanted births and increase in infant mortality, women additionally face risks of gender discrimination, sexual violence, early marriage and miscarriage and birth complications (19). The government of Bangladesh welcomed the Rohingyas and made substantial efforts to accommodate them but the GOB had clearly maintained from the beginning that asylum for the refugees was temporary and encouraged their immediate return, of the original 20 refugee camps that were constructed in 1992 in south -western Bangladesh, among them only two are remain near Nayapara refugee camp at Teknaf and Kutupalong refugee camp near Ukhia, giving shelter to 21,621 refugees, Kutupalong camp officially houses 8,216 refugees and Nayapara 13,405 as of December 2001(20).
Methods:
Study Place:
The study was conducted at the refugee camp in Cox’s Bazar in Bangladesh.
Data Collection, Management & Analysis
The data was collect from the refugee camp in Cox’s Bazar in Bangladesh through a standard mixed type questionnaire. The study was conducted at the Nayapara refugee camp at teknaf in Cox’s Bazar. About 149 samples were collected from July 2016 to October 2016 in Nayapara refugee camp. After collecting the data analysis is done by SPSS (Statistical Package of Social Science) software version 16.0.
Ethical consideration
A research proposal was submitted to the public health department of ASA University for approval and the proposal was approved by the faculty members and gave permission initially from the supervisor of the research project and from the academic coordinator before conducting the study. The necessary information has been approved by the ethical committee of public health department and was permitted to do this research. Also the necessary permission was taken from the Camp In charge (CIC), health coordinator & medical team leader of the refugee health unit (RHU). The participants were explained about the purpose and goal of the study before collecting data from the participants. Pseudonyms were used in the notes, transcripts and throughout the study. It was ensured to the participants that the entire field notes, transcripts and all the necessary information was kept in a locker to maintain confidentiality and all information was destroyed after completion of the study. The participants were also assured that their comments will not affect them about any bad thing.
Result:
Table 1: Distribution of demographic variables among the respondents (n=149)
|
Demographic Variable |
|||
|
Gender |
Gender |
Frequency |
Percent |
|
Male Female |
67 82 |
45 55 |
|
|
Age |
Age |
Frequency |
Percent |
|
01-10 11-20 21-30 31-40 41-50 51-60 61-70 71-80 81-90 91-100 101-110 |
06 10 14 35 29 23 18 10 2 1 1 |
4.0 6.7 9.3 23.5 19.5 15.4 12.1 6.7 1.4 0.7 0.7 |
|
|
Educational Status |
Educational level |
Frequency |
Percent |
|
Illiterate Literate |
112 37 |
75.2 24.8 |
|
|
Marital Status |
Marital Status |
Frequency |
Percent |
|
Married Unmarried Widow |
105 20 24 |
70.5 13.4 16.1 |
|
|
Occupations of the Participants |
Occupation |
Frequency |
Percent |
|
Fisher Man |
1 |
.7 |
|
|
Agriculture |
3 |
2.0 |
|
|
Driver |
2 |
1.3 |
|
|
Day laborer |
11 |
7.4 |
|
|
unemployed |
42 |
28.2 |
|
|
Housewife |
61 |
40.9 |
|
|
Student |
13 |
8.7 |
|
|
other (Specify) |
16 |
10.7 |
|
Among 149 participants 82 (55%) were female and 67 (45%) were male. Female were predominantly higher than male. Mean age of the participants was 45.52 (±19.28) years, mode was 35. The range is 100 with minimum age 02 years and maximum 102 years. Among the participants the higher numbers of the participants were at the age of 35 years and the numbers were 13 (8.7%). The number of ≤ 18 years were 15 (10.1%), ≤60 years were 102 (68.4%) and ≥60 were 32 (21.5%). Majority of the participants were illiterate the numbers were 112 (75.2%) and 37 (24.8%) participants were literate those who complete their primary education. Majority of the participants were married the numbers were 105 (70.5%) followed by those who are widow the numbers were 24 (16.1%) and 20 (13.4%) participants were married. Nuclear family were 76 (51%) whereas 72 (49.0%) participants were in extended family. Among total particepants housewife were 61(40.9%), Unemployed were 42 (28.2%), others 16 (10.7%), student 13(8.7%), Day labour 11(7.4%), Agriculture 3(2%) Driver2 (1.3%) and Fisher man1 (.7%).
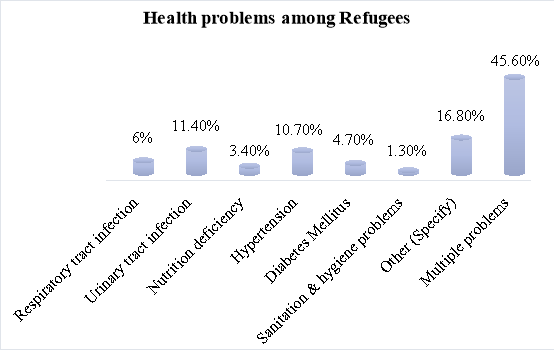 Figure -1: Health problems among the participants (n=149)
Figure -1: Health problems among the participants (n=149)
In this study 149 participants are gathered as sample, where there mean is 7.39 with standard deviation (± 3.28), median 9.0 and the mode was 10. Out of the 149 participants, 68 participants (45.6%) were had multiple problems followed by those had other specific problems 25 participants (16.8%) like musculoskeletal pain, visual problems and peptic ulcer. Urinary tract infection is the leading individual health problems among 17 participants (11.4%) had this problem, 16 (10.7%) participants had hypertension, 9 (6%) had respiratory tract infection, 5 (3.4%) had nutrition deficiency, 7 (4.75%) had diabetes mellitus and 2 (1.3%) had sanitation & hygiene problems.
Table 2: Type of health care and health care receive organization (n=149)
|
Type of health care |
Frequency |
Percentage |
|
Medicine Counseling Laboratory test Referral Nothing Multiple Services |
82 2 5 5 6 49 |
55.0 1.3 3.4 3.4 4.0 32.9 |
|
Health care receive organization |
Frequency |
Percentage |
|
Refugee Health unit (RHU) |
75 |
50.3 |
|
Handicap International (HI) |
1 |
0.7 |
|
Others |
6 |
4.0 |
|
Multiple Organizations (RHU, HI, ACF, RTMI) |
67 |
45 |
In this study among the 149 participants, 82 (55%) participants took medicine from RHU, 49 (32.9%) received multiple services like medicine, referral, laboratory test & others, 5 (3.4%) received both laboratory test & referral to other organizations & 6 (4%) participants said that they didn’t received any treatment from health center And majority of the participants said that they receive health services from RHU, the number was 75 (50.3%) followed by they received health services from multiple organizations like RHU, HI, ACF & RTMI and 6 (4%) said that they receive services from others like MSF, health complexes.
Table 3: Health care services that meet the demands and the reason for not fulfill the demands (n=149)
|
Health care services that meet the demands |
Frequency |
Percent |
|
Yes |
17 |
11.4 |
|
No |
45 |
30.2 |
|
Sometimes |
87 |
58.4 |
|
Reason that not fulfill the demands |
Frequency |
Percent |
|
Not enough medicine supply in the camps |
47 |
31.4 |
|
Narrow space in health unit |
5 |
3.4 |
|
Lack of doctors |
25 |
16.8 |
|
Other |
5 |
3.4 |
|
Not enough medicine & Lack of doctors |
50 |
33.6 |
Among the 149 participants, only 11.4% (n=17) participants said they have enough health services to meet their needs, 58.4% (n=87) said that sometimes they have enough health services to meet their needs and 30.2% (n=45) said that they have not enough health services to meet their needs and majority of the participants said they didn’t meet needs because there is a lack of medicine supply & doctors in the camps the number was 50 (33.6%) and 47 (31.4%) patients said that they didn’t meet needs because there is a lack of medicine supply in camps.

Figure – 2: Expectation among the participants (n=149)
Among the 149 participants, 56 (37.6%) participants said that they were need better services, majority of the participants said that they need multiple services includes more laboratory test, radiological imaging, more medicine & more doctors, 17 (11.4%) participants said that they need more medicine and 3 (2%) said that they require more referral, laboratory test & radiological imaging.

Figure – 3: Satisfaction level among the participants (n=149)
Among the 149 participants, only 16.1% (n=24) participants were satisfied with the quality of service received, 56.4% (n=84) said that they were sometimes satisfied after received services and 27.5% (n=41) said that they were not satisfied after received services.
Discussion:
The result of this study showed that 45.6% participants were had multiple problems followed by 16.8% participants had other specific problems like musculoskeletal pain, visual problems and peptic ulcer. Urinary tract infection is the leading individual health problems, among the participants 11.4% had this problem, 10.7% participants had hypertension, 6% had respiratory tract infection, 3.4% had nutrition deficiency, 4.75% had diabetes mellitus and 1.3% had sanitation & hygiene problems during the course of the study and also in this study it was found that among the participants the mean age of the participants was 45.52 (±19.28) years. The range is 100 with minimum age 02 years and maximum 102 years. Among the participants the higher numbers of the participants were at the age of 35 years 8.7%. The numbers of ≤ 18 years were 10.1%, ≤60 years were 68.4% and ≥60 were 21.5%, the middle age people had mostly health problems. Ã-nen C et al stated that health problems among refugees were frequently seen mostly at the early childhood & in adult aged problems, a community based study was carried out by Turkish medical association stated that 25.0% children had sleeping disorder at the of below 18 years & 24.0% have adult persons with the same problems (22).
The study showed that, majority of the participants said that they receive health services from RHU, the number was 75 (50.3%) followed by they received health services from multiple organizations like RHU, HI, ACF & RTMI and 6 (4%) said that they receive services from others like MSF, health complexes.
The study showed that, only 16.1% participants were satisfied with the quality of service they received, 56.4% said that they were sometimes satisfied after received services and 27.5% said that they were not satisfied after received services, Among the 149 participants, 32.9% participants said that they were not satisfied because there is a lack of medicine supply in RHU, 13.4% participants were not satisfied because there is a lack of qualified doctor in RHU & 38.9% participants stated that in RHU there is a lack of budget, lack of doctor, lack of medicine supply, lack of referral to other organization in timely, not gave proper medicine & treatment & lack of serial maintain during medicine collection that’s why they were not satisfied.
Conclusion
From the above discussion it can be said that Rohingya refugees are not having rights to live as human being. Considering the importance of nationality crisis of the Rohingya and problems associated with these following steps can be taken: Supplies of adequate Medicine, Increase Doctors’ and Nurse, Modernized treatment, Increase Childcare hospital, Decrease pollution, Mass awareness of life threatening disease.
Acknowledgement: Author acknowledges the Kauvery Research Group for necessary support.
Funding: Self funded
Conflict of Interest: None
References:
- Azad A, Jasmin F. Durable solutions to the protracted refugee situation: The case of Rohingyas in Bangladesh. J Indian Res. 2013;1(4):25-35.
- Teng TS, Zalilah MS. Nutritional status of rohingya children in kuala lumpur. Malaysian J Med Heal Sci. 2011;7(1):41-9.
- The Rohingya Refugee Situation in Bangladesh Evan Coutts American International School / Dhaka Senior Project 2005. 2013;1-37.
- UNHCR & WFP. Report of the WFP-UNHCR Joint Assessment Mission, Bangladesh. Assessment. 2010;(June).
- Kemmer TM, Bovill ME, Kongsomboon W, Hansch SJ, Geisler KL, Cheney C, et al. Iron deficiency is unacceptably high in refugee children from Burma. J Nutr. 2003;133(12):4143-9
- Department of Sociology University of Dhaka Nationality crisis and Rights of Rohingya Refugee Children : A Sociological Analysis of Children ‘ s Rights in Bangladesh. 2014;2011-2.
- UNHCR. Bangladesh: Analysis of Gaps in the Protection of Rohingya Refugees. 2007;(May).
- Kiragu Angela Li Rosi Tim Morris E. UNITED NATIONS HIGH COMMISSIONER FOR REFUGEES States of denial A review of UNHCR’s response to the protracted situation of stateless Rohingya refugees in Bangladesh. 2011;(December).
- Karaman MA, Ricard RJ. Meeting the Mental Health Needs of Syrian Refugees in Turkey. 2016;6(4):318-27.
- Eastern M, Studies S. OrtadoğuStrateji̇k AraştirmalarMerkezi̇ Center for Middle Eastern Strategic Studies. 2015.
- TTB. War, Migration and Health; Experience of Turkey.
- Red Cross. Children affected by armed conflict (CABAC). 2000;(September):48-51.
- Gazi R, Mercer A, Wansom T, Kabir H, Saha NC, Azim T. An assessment of vulnerability to HIV infection of boatmen in Teknaf, Bangladesh. Confl Health. 2008;2:5.
- Holland MSF, Fronti S, March H. 10 Years for the Rohingya Refugees in Bangladesh : Past , Present and Future. 2002;(March):1-45.
- Socio-economic and family planning aspects of rural people in Bangladesh : A case study of Comilla District. 2014;6(10):348580.
- Farzana KF. Music and Artistic Artefacts: Symbols of Rohingya Identity and Everyday Resistance in Borderlands. Austrian J South – East Asian Stud [Internet]. 2011;4(2):215-36.
- Genocide IS, In O. Persecution of the Rohingya Muslims : Persecution of the Rohingya Muslims. 2015;(October).
- Herald M. Refugee Health- Research Barriers to access to health care for newly resettled Refugee Health – Research. 2006;185(11).
- Sharara SL, Kanj SS. War and infectious diseases: challenges of the Syrian civil war. PLoS Pathog. 2014;10(10):e1004438.
- Cheung S. “Migration control and the solutions impasse in South and Southeast Asia: Implications from the Rohingya experience.” J Refug Stud. 2012;25(1):50-70.
- AFAD. Population influx from Syria to Turkey life in Turkey as a Syrian guest. 2014. 2014;(1):152.
- Ã-nen C, GüneÅŸ G, Türeme A, AÄŸaç P. Depression and Anxiety Case among in Syrians that Live in a Refugee Camp. The Journal of Academic Social Science. 2014;2(6):223-30.