Solid Variant of Aneurysmal Bone Cyst of Thoracic Spine
SOLID VARIANT OF ANEURYSMAL BONE CYST (S-ABC) OF THORACIC SPINE: A Case Report
Abstract
Introduction: The solid variant of aneurysmal bone cyst (ABC) has been seen on occasional basis, and till date very few cases involving the spine has been reported. The utmost difficulty is in diagnosing it with X-rays without using biopsy or surgery methods. In this case report, we present a very rare tumor of thoracic spine which was presented to us in an emergency situation and was managed by 360 degree decompression via posterior only approach and stabilization.
Case Report: A 16-year-old young boy, presented to us with a sudden onset of weakness in both the lower extremities leading to paraplegia. He also had a history of back and chest pain since a year. Collapse of T5 vertebrae on plain radiograph was observed. The patient was taken to the operating room on emergency basis with an initial plan of a total en-block spondylectomy of T5. However, intraoperatively, histology favored solid-ABC variant rather than spindle cell tumor, Giant Cell Tumor. Thus Initial plan was revised to 360 degree decompression and without resecting body en-block via posterolateral approach.
Results: After surgery, there was not only complete resolution of sensory and motor functions but also his chest and back pain was resolved. The diseased vertebral body was re-constituted with new bone formation and healing was seen at 18 months, postoperatively.
Conclusion: This case report concludes that solid ABC should be kept as a differential diagnosis for tumour of spine. Intraoperative frozen sections shall be useful as well. However,early diagnosis and appropriate surgical plays the most important role in successful management of ABC.
Keywords: Aneurysmal Bone Cyst, ABC, Osteolytic lesion, Palliative Surgery.
INTRODUCTION
The solid variant of aneurysmal bone cyst (ABC) is generally very rare to see and accounts for 3.4% to 7.5% of all aneurysmal bone cysts [1]. It is an expansile cystic lesion which can occur in any part of the bone and most often affects individuals in their second decade of life [2,3].
Jaffe and Lichtenstein were the first ones to describe ABC as its own entity in 1942, when they noted “a peculiar blood-containing cyst of large size.” [4]. Although benign, an ABC can grow rapidly and destruct the bone. Its expansile nature can cause lot of swelling, pain, deformity, disruption of growth plates, pathologic fractures and neurologic symptoms depending on location [2,3].
As many as 69% of primary ABCs demonstrate a characteristic clonal t(16;17) genetic translocationwhich can lead to upregulation of the TRE17/USP6 oncogene [5,6].
However, the diagnosis of ABC is quite difficult without biopsy or surgery. There is a distinct solid variant of ABC which was first described by Sanerkin et al., in 1983 [7]. This solid variant may be easily misdiagnosed as a spindle cell tumor, especially osteosarcoma [1].
ABCs are generally treated with surgery. However, asymptomatic ABCs may also exist which is characterized by clinically insignificant destruction of the bone. In such cases, close monitoring alone of the lesion is sufficient enough. However, the diagnosis must be first confirmed and the lesion should not be increasing in size. In case monitoring alone is selected as the management plan [8].
CASE REPORT
A 16-year-old young boy, presented to us with a sudden onset of weakness in both the lower extremities leading to paraplegia. He also had a history of back and chest pain since a year. A good rectal tone without any perineal anesthesia was seen in rectal examination and the post-void residual urine volume was negligible. His premedical history was unremarkable. Laboratory findings were all within normal limits. Plain radiograph revealed collapse of T5 vertebrae in figure 1.
CT axial images showed expansile and lyrics lesion in vertebral body, left pedicle and transverse process. T2-weighted Sagittal and axial MRI T2 weighted images of thoracic spine showing hyperintence signals in T5 vertebral body, left pedicle and transverse process with pathological fracture (Figure 2).
Attempt to establish preoperative tissue biopsy couldn’t be done because of the urgency of decompression. The patient was taken to the operating room on emergency basis with an initial plan of a total en-block spondylectomy of T5.
However, intraoperatively, histology favored solid-ABC variant rather than Giant Cell Tumor. Thus Initial plan was revised to palliative surgery with 360 degree decompression and without resecting body en-block via posterolateral approach as shown in figure 3. The vertebral column was reconstructed in a 360° manner with an expandable titanium cage and pedicle screw fixation (Figure 3).
Results
After surgery, there was not only complete resolution of sensory and motor functions but also his chest and back pain was resolved. The diseased vertebral body was re-constituted with new bone formation and healing was seen at 18 months, postoperatively (figure 4).
Discussion
ABCs are benign, but locally aggressive and highly vascular tumors which has recurrence rates after curettage of equal to or less than 50 % [9]. However, Malghem had reported in his study about the spontaneous healing in three patients [10].
ABCs are found to have a predilection for the lumbar spine in the case series presented by Boriani [11]. Although CT and MRI are preferred diagnostic methods, it may be noted that in the literature, biopsy is the utmost necessary for confirmation, due to similarity of many bone lesions in appearance. Biopsy will show the proliferating round or oval cells, generally mixed with randomly distributed multi-nucleated giant cells, regions of reactive fibroblastic proliferation and region of tumor with the blood filled microcystic component [12].
Depending on the proliferative component, the solid variant of ABC may be histologically misdiagnosed for other benign or malignant tumor-like lesions of the bone [1].
The pathological differential diagnosis should always be kept in mind while thinking of ABC. They include solitary bone cyst, giant cell tumor, hemangioma, osteosarcoma, and chondroblastoma [13].
Treatment of ABC is also very controversial which includes arterial embolization, curettage with or without bone grafting, complete excision, intra-lesional drug injections (steroid and calcitonin) and radiation [14]. However,early diagnosis and appropriate surgical plays the most important role in successful management of ABC [15].
Whether surgical management results in a better outcome and recurrence rate than a more conservative or palliative one (for example, curettage alone) remains controversial and to be seen in future studies.
Conclusion
This case report concludes that ABC should be kept as a differential diagnosis for tumour of spine. Intraoperative frozen sections shall be useful as well. An effective spinal decompression and stabilization of ABC can be achieved by partial or subtotal excisions. However,early diagnosis and appropriate surgical plays the most important role in successful management of ABC.
References
- Bertoni F, Bacchinin P, Capanna R, Ruggieri P, Biagini R, Ferruxxi A, Bettelli G, Picci P, Campanacci M: Solid variant of aneurysmal bone cyst. Cancer 1993, 71:729-734.
- Clayer M. Injectable form of calcium sulphate as treatment of aneurysmal bone cysts. ANZ J Surg. 2008 May. 78(5):366-70.
- Burch S, Hu S, Berven S. Aneurysmal bone cysts of the spine. Neurosurg Clin N Am. 2008 Jan. 19(1):41-7.
- Jaffe HL, Lichtenstein L. Solitary unicameral bone cyst with emphasis on the roentgen picture, the pathologic appearance and the pathogenesis. Arch Surg. 1942. 44:1004-25.
- Panoutsakopoulos G, Pandis N, Kyriazoglou I, Gustafson P, Mertens F, Mandahl N. Recurrent t(16;17)(q22;p13) in aneurysmal bone cysts. Genes Chromosomes Cancer. 1999 Nov. 26(3):265-6.
- Lau AW, Pringle LM, Quick L, Riquelme DN, Ye Y, Oliveira AM, et al. TRE17/ubiquitin-specific protease 6 (USP6) oncogene translocated in aneurysmal bone cyst blocks osteoblastic maturation via an autocrine mechanism involving bone morphogenetic protein dysregulation. J Biol Chem. 2010 Nov 19. 285(47):37111-20.
- Sanerkin NG, Mott MG, Roylance J: An unusual intraosseous lesion with fibroblastic, osteoclastic, osteoblastic, aneurysmal and fibromyxoid elements: “solid” variant of aneurysmal bone cyst. Cancer 1983, 51:2278-2286.
- Tedesco N. Medscape, Aneurysmal Bone Cyst. Available from: http://emedicine.medscape.com/article/1254784-overview#a11. Accessed on 24th January, 2017.
- Ruiter DJ, Van Rijssel TG, Van Der Velde EA. Aneurysmal bone cysts: a clinicopathological study of 105 cases. Cancer. 1977;39:2231-2239. doi: 10.1002/1097-0142(197705)39:5<2231::AID-CNCR2820390541>3.0.CO;2-Q.
- Malghem J, Maldague B, Esselinckx, Noel H, De Nayer P, Vincent A. Spontaneous healing of aneurysmal bone cysts: a report of three cases. J Bone Joint Surg Br. 1989;71B:645-650.
- Boriani S, De Iure F, Campanacci L, et al. Aneurysmal bone cyst of the mobile spine: report on 41 cases. Spine. 2001;26:27-35. doi: 10.1097/00007632-200101010-00007.
- Saccomanni R. Aneurysmal bone cyst of spine: a review of literature. Arch Orthop Trauma Surg. 2008;128:1145-1147. doi: 10.1007/s00402-007-0477-6.
- Hay MC, Paterson D, Taylor TK. Aneurysmal bone cysts of the spine. J Bone Joint Surg Br. 1978;60:406-411.
- Tsai JC, Dalinka MK, Fallon MD, Zlatkin MB, Kressel HY. Fluid-fluid level: a nonspecific finding in tumors of bone and soft tissue. Radiology. 1990;175(3):779-782.
- Garg S, Mehta S, Dormans JP. Modern surgical treatment of primary aneurysmal bone cyst of the spine in children and adolescents. J Pediatr Orthop. 2005;25(3):387-392. doi: 10.1097/01.bpo.0000152910.16045.ee.
Figures and Legends

Figure 1. Radiograph showing collapse of T5 Vertebra (AP and LAT XRAY of thoracic spine showing pathological fracture and collapse of T5)

FIGURE 2. CT (Top Left) & MRI (Bottom left and Right).
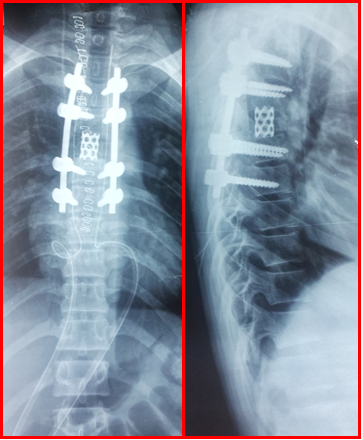
Figure 2. Intraoperative AP and Lat X-ray of thoracic spine showing pedicle screw fixation and cage

Figure 4. Post-surgery MRI showing new bone formation