Immediate and Late Effect of Cryotherapy on Balance
immediate and late effect of cryotherapy on balance IN HEALTHY SUBJECTs
Abstract
Background: cryotherapy application is commonly used as a physical therapy tools with many known advantage, however several research have reported decrease in subject balance which affect quality of movement following cryotherapy application, therefore the purpose of study to investigate the immediate and late effect of cryotherapy on ankle dominant joint on static balance and test the difference in static balance change between both sexes. Methods: thirty normal subjects, Subjects had their static balance tested during two conditions: (1) an experimental condition where the subject received the cryotherapy application by using cooled gel pack to the dominant ankle joint for 15 minutes immediately before static balance testing and (2) a control condition finished at room temperature. The order of testing condition was randomized by using a coin flip. Biodex balance system was used to measure static balance. Result: analysis of data using ANOVA and unpaired test ,show insignificantly statistically effect in all aspect of static balance within female group with p value of overall stability index =0.669,Anterior/posterior stability index =0.196 and medial/lateral stability index =0.989,insignificantly statistically effect in all aspect of static balance within male group with p value of overall stability index =0.382,Anterior/posterior stability index =0.552 and Medial/lateral stability index =0.46 and insignificant statistically difference between male and female in all aspect of static balance. Conclusion: The result of current study suggest that fifteen minutes of cold gel pack on ankle dominant extremity have no effect on static balance on both sexes .
Key words: static balance, cryotherapy
Introduction:
cryotherapy therapy is a popular non-pharmacological intervention, The term “cryotherapy” was used in year 1908 by A.W. Pusey to describe the treatment of skin injuries with low temperatures[1,2] , The primary aim of cryotherapy is the removal of heat energy from the site of injury, in order to facilitate a therapeutic effect [3] by produces a number of physiological effects to the human body including a reduction in blood flow, edema, hemorrhage[4], cellular metabolic rate, hypoxia, enzymatic activity and tissue damage[5]. Cryotherapy has also been demonstrated to significantly increase the pain threshold and pain tolerance by reducing nerve conduction velocity and muscle spasm [6].
Cryotherapy often used in athletic and rehabilitation cases to manage injury during the immediate and rehabilitative phases [7]. Cryotherapy treats the muscle damage caused by High-intensity exercise including predominantly eccentric activity, unaccustomed activity, and exercise of long duration and/or high intensity which has been shown to induce an inflammatory response [8].
In spite of the characterized treatment advantage of cryotherapy, there are reduction in subjects performance variables are likely to occur after returning to normal movement immediately after cryotherapy application,[9]especially , decrease speed of running, muscle strength speed and agility measures have been noted after cryotherapy application over many anatomical areas and studies[10,11].
The ability to conserve postural control or balance is important for the correct carrying out of all daily activity ranging from standing and walking to sitting and standing from a chair [12]. Possessing the ability to conserve several positions, to react automatically to voluntary movements of the body, and to react to external disturbance represents a postural control domain needed in daily life [13].
The maintenance of balance is important in the prevention of injuries and this ability depends on proprioceptive input from capsuloligamentous and musculotendinous mechanoreceptors in combining with vestibular and visual input to the central nervous system (CNS)[14,15] . This input used in feedback and feed-forward loops to provide the proper neuromuscular response [16-17]. Variations in any of these inputs would disturb balance and increase the risk of injury [18].
There is also growing awareness that rehabilitation using cryotherapy has deleterious effects on balance, or return patients to their previous functional levels [19, 20].Quality of movement is important as strength of movement, and the key of movement quality is balance [21]. Even if a patient has regained full strength and range of motion, if they still have poor balance and proprioception, they are at risk for re-injury.
During the management of acute distortion, cryotherapy is commended after the injury and in rehabilitation, ice application is supposed to promote the beginning of active exercise and its progression [7]. In practice it can happen that sportsmen are sent back to exercising or competition immediately after cryotherapy. Although the question is controversially discussed, if physical activities after ice application can be re-established without risk or increase liability to injury. This study takes up the problems if cryotherapy application at the ankle disrupts static balance so that an increased risk of injury could result and the study also clarify the immediate and late effect and test the difference in static balance between both sex.
Methodology
The current study was conducted at biomechanics laboratory at faculty of physical therapy, modern university, in the period from December 2015 to April 2016 to investigate the immediate and late effect of cryotherapy application on dominant ankle joint on static standing balance and test the difference in static balance between both sexes.
Design of study
Cross over (single repeated measurements) design used in this study to determine the immediate and late effect of cryotherapy application on dominant ankle joint on static standing balance and test the difference in the static standing balance between both sexes.
Subjects
A sample of thirty healthy normal subjects (fifteen male and fifteen female), subjects were recruited using publically distributed posters and by online social media. Subjects had their static balance examined during two situations: (1) an experimental situation where the subject received the cryotherapy application by using cooled gel pack to the dominant ankle joint for fifteen minutes immediately before static balance testing and (2) a control situation finished at room temperature. The order of examining situation was randomized by using a coin flip. Participant finished the control situation first immediately finished the experimental situation following assessment. Participants randomized to the cryotherapy situation first had the control session arranged at a separate time to confirm no lingering effects remain from the cryotherapy procedures.
Subjects participate in the current study after approval of ethical committee of faculty of physical therapy, Cairo University with number P.T.REC/012/001035 and all subjects provided written informed consent. Subjects were included if their age range from 18 to 40 years [22] free from musculoskeletal diseases and neurological diseases affecting the lower limb. Excluded if had musculoskeletal disorders in lower limb, had infected skin diseases and loss of sensation, had Metabolic or vascular disease with neurological component such as diabetes, had previous ankle operation and had recent injury of ankle joint.
Instrumentation
- Measurement instrumentation
The device used in this study (Biodex Medical Systems Inc., Shirley, New York, USA) was a foot platform (circular in shape with a diameter of 21.5΄, which permits up to 20° tilting from horizontal in all directions), support rails that were adjustable from 25΄ to 36.5΄ above the platform, and could be swung away if desired, a display module whose height was adjustable from 53΄ to 68΄ above the platform and angle was adjustable from vertical back to 45°, with a display viewing area of 24.8 Ã- 18.4 cm and a printer. This testing machine has 12 dynamic levels plus locked for static measurements [23].
Stability indexes
the stability index represents the variance of platform displacement in degrees from level. An increase in number indicate considerable motion, which indicates a problem with balance [24] . The participant’s ability to control the platform’s angle of tilt was measured by the system and noted as a stability index. The data on the balance of the tested participants were supplied to the system. These data included anteroposterior stability index (APSI), mediolateral stability index (MLSI), and overall stability index (OSI). The smaller the amount of sway, the lower the numerical value of these indexes [24].
- OSI: represented the variance of foot platform displacement in degrees, from level, in all motions during the test. A high number was indicative of considerable movement during this test.
- APSI: represented the variance of foot platform displacement, in degrees, from level, for motion in the sagittal plane.
- MLSI: represented the variance of foot platform displacement, in degrees from level, for motion in the frontal plane [24] .
- Therapeutic instrumentation:
Reusable cold gel pack 25.4 x 48.1 cm. 5 +/- degree C [25] was frozen and wrapped with a towel and supported with elastic strap around the ankle joint of dominant lower extremity.
Procedure
Each participant received a verbal explanation about the test steps. When the system was on, the first displayed screen was the main menu. It allowed us to choose entering testing, training, or system utilities. Choosing to enter testing showed the next screen, which allowed determination of the test parameters such as test duration and the stability level chosen. The weight and height of the participant were recorded and the next screen was used for the centering process. The next screen was the stability test screen, where the start key was pressed to lock or unlock the platform and begin the test. A cursor appeared during the test tracing the movement of the platform while the clock counted till the time of the test ends. The next screen showed a menu. The examiner chooses the numeric report option on this screen to allow the participant’s numeric screen appear. Pressing start while on this screen initiates printing of the report, which includes the numeric values of the APSI, MLSI, and OSI (operation and service manual).
Step 1: balance assessment
the participants were tested without footwear and asked to perform two test trials before a specific test condition for the purpose of instrument familiarity before data collection. Then, the participant was first asked to assume the test position (standing on dominant foot) with arms held at the sides, eye closed and to attempt to control his/her balance as much as possible. Each participant was asked to center him/herself on the foot platform before starting the test.
The test parameters introduced into the device were:
- Participant’s age , weight and height
- Stability level: all participants were tested on stability level 0 for 15 s.
Then, the start key was pressed in the control panel (which took 5 s) with an auditory alarm just before the beginning of the test. The participant was instructed that the test was started just after the alarm. Each participant was instructed to maintain his/her balance for the period of the test. Three trials were performing prior to the measurement.
There was report obtained at the end of each test include information on OSI, APSI, and MLSI.
Step 2: cryotherapy application
Reusable cold gel pack 25.4 x 48.1 cm. 5 +/- degree C was employed as the cryotherapy modality in this study. Application duration will be 15 minutes. Wrapping of pack by towel will applied all around ankle joint of domain extremity with towel in between .Two elastic straps will used to secure the ice pack. The subject will asked to relax during cryotherapy application to limit activity of muscle and lessen any change in temperature of tissue.
Step 3: balance reassessment
the participant was asked to repeat the same balance testing procedures directly after cryotherapy application, 30 minutes later and 60 minutes later to measure post OSI, MLSI, and APSI.
Statistical analysis
All statistical analysis were carried out by using SPSS,version 23 for windows; SPSS Inc., Chicago,Illinois,USA.the normality of data distribution was tested through the Shapiro-wilk test.Descriptive data for participants, characteristics was calculated as “the mean, standard deviation and range “minimum & maximum” of measured variables, ANOVA tests used to compare between pretest and posttest. Unpaired test used to compare between male and female. Level of significant will set at <0.05.
Results:
General characteristics of the subjects:
In this study, thirty subjects were assigned randomly, the range of the ages is between 18 to 40 years overall. There was no statistically significant differences between the groups in their ages as the p-value are 0.412. The range of the weight is between 50 to 105 kg. There was no statistically significant differences between the groups in their weight as the p-value are 0.214. The range of the Height is between 156 to 195 cm. There was no statistically significant differences between the groups in their weight as the p-value are 0.366.
Table (1): Demographics Distribution
|
Items |
Male |
Female |
Comparison |
Significant |
|
|
Mean±SD |
Mean±SD |
T-value |
P-value |
||
|
Age (years) |
26.4 ± 6.08 |
25.533 ± 5.41 |
0.412 |
0.682 |
No Significant |
|
Weight (Kg) |
70.89 ± 14.57 |
77.2 ± 5.41 |
-1.270 |
0.214 |
No Significant |
|
Height (cm) |
165.27 ± 4.57 |
166.66 ± 6.41 |
-0.411 |
0.366 |
No Significant |
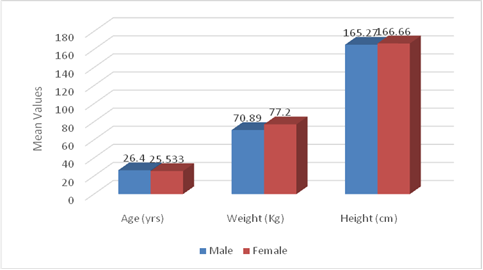
Figure. (1): Demographics Distribution
As for the gender distribution, 15 subjects (50%) were male and 15 subjects (50%) were females. In addition, 26 subjects (86.7%) had their dominant right leg tested, and 4 subjects (13.3%) had their dominant left leg tested.
Static Balance
- Pre-test
The results are shown using the following table (2) and illustrated in figure (2).
1) Overall Stability Index
Independent t-test was used to show difference between pretest for females and males. The female mean value of overall stability index (3.471.42) was significantly different from (5.042.31) with t test = -2.242 and p value = 0.033*.
2) A/P Stability Index
Independent t-test was used to show difference between pretest for females and males. The female mean value of A/P Stability index (2.41  0.85) was significantly different from (3.3931.65) with t test = -2.157 and p value = 0.043.
3) M/L Stability Index
Independent t-test was used to show difference between pretest for females and males. The female mean value of M/L Stability index (2.01  1.08) was insignificantly different from (2.991.72) with t test = -1.887 and p value = 0.072.
Table (2): The pre-test results for the Stability Indices – Static
|
Stability Index |
Overall Stability Index |
A/P Stability Index |
M/L Stability Index |
|
Pre-test for Females |
3.671.41 |
2.4070.85 |
2.011.08 |
|
Pre-test for Males |
5.042.3 |
3.391.65 |
2.991.72 |
|
Independent t-value p value |
-2.492 0.033* Significant |
-2.157 0.045* Significant |
-1.884 0.072 Insignificant |
Data are expressed as mean ± SD.
P> 0.05= insignificant.
*P< 0.05= Significant.
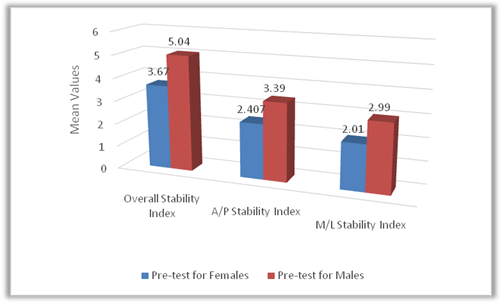
Figure (2): The pre-test results for the Stability Indices – Static
B) Within Group (Females)
The results are shown using the following table (3) and illustrated in figure (3).ANOVA F-test was used to show difference between pre and post-test in the stability indices.
- Overall Stability Index:
The mean value was pretest (3.471.42) when compared with its corresponding no significant difference after assessment immediately (3.781.868), after 30 minutes (3.41  2.27), and after 60 minutes (4.29  2.86) with f test = 0.521 and p value = 0.66.
- A/P Stability Index:
The mean value was pretest (2.41  0.85) when compared with its corresponding no significant difference after assessment immediately (2.47  1.52), after 30 minutes (2.14  1.27), and after 60 minutes (3.27  1.43) with f test = 1.616 and p value = 0.196.
- M/L Stability Index:
The mean value was pretest (2.01  1.08) when compared with its corresponding no significant difference after assessment immediately (2.2  1.07), after 30 minutes (2.12  1.84), and after 60 minutes (2.13  1.98) with f test = 0.04 and p value = 0.989.
Table (3): The mean values and S.D of Stability Indices before starting and after the test for Females – Static
|
Data of evaluations |
Overall Stability Index |
A/P Stability Index |
M/L Stability Index |
|
Pre-test |
3.47  1.42 |
2.41 0.85 |
2.01 1.08 |
|
Post-Immediate |
3.73  1.868 |
2.47 1.52 |
2.2 1.07 |
|
Post-30 minutes |
3.41  2.27 |
2.141.27 |
2.12 1.84 |
|
Post-60 minutes |
4.29  2.86 |
3.27 1.43 |
2.13 1.98 |
|
F-value ANOVA |
0.521 |
1.616 |
0.04 |
|
p value |
0.669 Insignificant Difference |
0.196 Insignificant Difference |
0.989 Insignificant Difference |
Data are expressed as mean ± SD.
P> 0.05= insignificant.
*P< 0.05= Significant; **P< 0.01= highly significant.
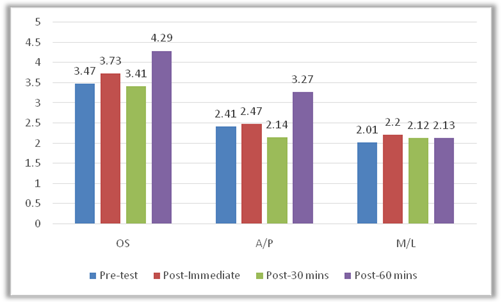
Figure (3): The mean values and S.D of Stability Indices before starting and after the test for Females – Static
D) Within groups (Males)
The results are shown using the following table (4) and illustrated in figure (4). ANOVA F-test was used to show the difference between post-test in the stability indices.
- Overall Stability Index:
The mean value was pretest (5.042.3) when compared with its corresponding no significant difference after assessment immediately (5.01 1.765), after 30 minutes (4.422.22), and after 60 minutes (3.951.56) with f test = 1.039and p value = 0.382.
- A/P Stability Index:
The mean value was pretest (3.391.69) when compared with its corresponding no significant difference after assessment immediately (3.41.42), after 30 minutes (3.11 1.78), and after 60 minutes (2.67 1.416) with f test = 0.707and p value = 0.525.
- M/L Stability Index:
The mean value was pretest (2.99 1.72) when compared with its corresponding no significant difference after assessment immediately (3.021.28), after 30 minutes (2.52 1.55), and after 60 minutes (2.33 1.02) with f test = 0.874and p value = 0.46.
Table (4): The mean values and S.D of Stability Indices before starting and after the test for Males – Static
|
Data of evaluations |
Overall Stability Index |
A/P Stability Index |
M/L Stability Index |
|
Pre-test |
5.042.31 |
3.391.65 |
2.99 1.72 |
|
Post-Immediate |
5.01 1.765 |
3.4 1.42 |
3.02 1.28 |
|
Post-30 minutes |
4.42 2.229 |
3.11 1.78 |
2.52 1.55 |
|
Post-60 minutes |
3.951.56 |
2.67 1.42 |
2.33 1.02 |
|
F-value ANOVA |
1.039 |
0.707 |
0.874 |
|
p value |
0.382 Insignificant Difference |
0.552 Insignificant Difference |
0.46 Insignificant Difference |
Data are expressed as mean ± SD.
P> 0.05= insignificant.
* P< 0.05= Significant; ** P< 0.01= highly significant.
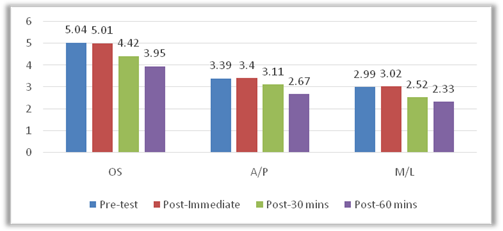
Figure (4): The mean values and S.D of Stability Indices before starting and after the test for Males – Static
D) Post test results – Static
The results are shown using the following table (5) and illustrated in figure (5). Independent t-test was used to show difference between post-test in the stability indices.
1) Overall Stability Index
Independent t-test was used to show difference between immediately post-test for females and males. The female mean value of overall stability index (3.73 ± 1.868) was insignificantly different from (5.01 ± 1.765) with t test = -1.913and p value = 0.063.
Independent t-test was used to show difference between 30 minutes post-test for females and males. The female mean value of overall stability index (3.41 ± 2.27) was insignificantly different from (4.42 ± 2.229) with t test = -1.227and p value = 0.23.
Independent t-test was used to show difference between 60 minutes post-test for females and males. The female mean value of overall stability index (4.29 ± 2.86) was insignificantly different from (3.95 ± 1.56) with t test = 0.415 and p value = 0.682.
|
Stability Index |
Immediate |
30 Minutes |
60 Minutes |
|
|
Overall Stability Index |
Post-test for Females |
3.73 ± 1.868 |
3.41 ± 2.27 |
4.29 ± 2.86 |
|
Post-test for Males |
5.01 ± 1.765 |
4.42 ± 2.229 |
3.95 ± 1.56 |
|
|
Independent t-value p value |
-1.913 0.063 Insignificant |
-1.227 0.23 Insignificant |
0.415 0.682 Insignificant |
Table (5.a): The mean values and S.D of Overall Stability Index post-test for both Females and Males-Static
Data are expressed as mean ± SD.
P> 0.05= insignificant.
* P< 0.05= Significant; ** P< 0.01= highly significant.
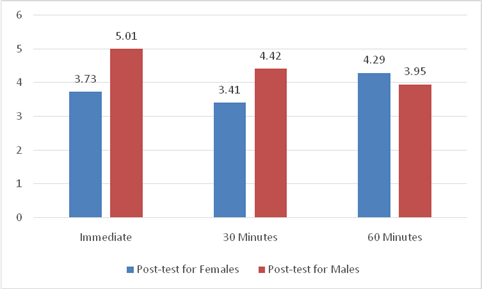
Figure (5.a): The mean values and S.D of Overall Stability Index post-test for both Females and Males-Static
2) A/P Stability Index
Independent t-test was used to show difference between immediate post-test for females and males. The female mean value of A/P Stability index (2.47 ± 1.52) was insignificantly different from (3.4 ± 1.42) with t test = -1.699and p value = 0.1.
Independent t-test was used to show difference between 30 minutes post-test for females and males. The female mean value of A/P stability index (2.14 ±1.27) was insignificantly different from (3.11 ± 1.78) with t test = -1.723and p value = 0.096.
|
A/P Stability Index |
Immediate |
30 Minutes |
60 Minutes |
|
|
A/P Stability Index |
Post-test for Females |
2.47 ± 1.52 |
2.14 ± 1.27 |
3.27 ± 1.43 |
|
Post-test for Males |
3.4 ±1.42 |
3.11 ± 1.78 |
2.67 ± 1.42 |
|
|
Independent t-value p value |
-1.699 0.1 Insignificant |
-1.723 0.096 Insignificant |
-0.925 0.363 Insignificant |
Independent t-test was used to show difference between 60 Minutes post-test for females and males. The female mean value of A/P stability index (3.27 ± 1.43) was insignificantly different from (2.67 ± 1.42) with t test = -0.925 and p value = 0.363.
Table (5.b): The mean values and S.D of A/P Stability Index post-test for both Females and Males-Static
Data are expressed as mean ± SD.
P> 0.05= insignificant.
* P< 0.05= Significant; ** P< 0.01= highly significant.
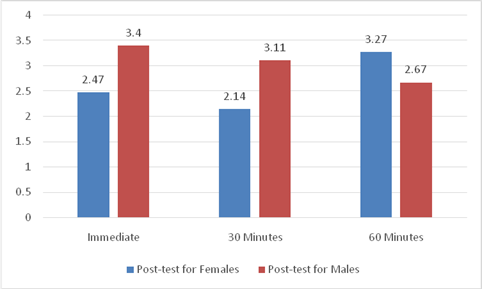
Figure (5.b): The mean values and S.D of A/P Stability Index post-test for both Females and Males-Static
3) M/L Stability Index
Independent t-test was used to show difference between immediate post-test for females and males. The female mean value of M/L Stability index (2.2±1.07) was insignificantly different from (3.02 ± 1.28) with t test = -1.898and p value = 0.068.
Independent t-test was used to show difference between 30 Minutes post-test for females and males. The female mean value of M/L stability index (2.12 ± 1.84) was insignificantly different from (2.52 ± 1.55) with t test = -0.656and p value = 0.518.
Independent t-test was used to show difference between 60 Minutes post-test for females and males. The female mean value of M/L stability index (2.13 ± 1.98) was insignificantly different from (2.33 ± 1.02) with t test =0.097and p value = 0.729.
Table (5.c): The mean values and S.D of M/L Stability Index post-test for both Females and Males-Static
|
M/L Stability Index |
Immediate |
30 Minutes |
60 Minutes |
|
|
M/L Stability Index |
Post-test for Females |
2.2 ± 1.07 |
2.12 ± 1.84 |
2.13 ±1.98 |
|
Post-test for Males |
3.02 ± 1.28 |
2.52 ± 1.55 |
2.33 ± 1.02 |
|
|
Independent t-value p value |
-1.898 0.068 Insignificant |
-0.656 0.518 Insignificant |
0.097 0.729 Insignificant |
Data are expressed as mean ± SD.
P> 0.05= insignificant.
* P< 0.05= Significant; ** P< 0.01= highly significant
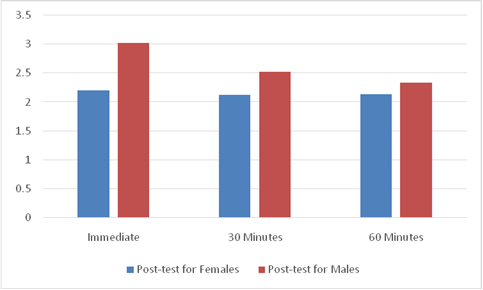
Figure (5.c): The mean values and S.D of M/L Stability Index post-test for both Females and Males-Static
Discussion:
The purposes of the study were To determine the immediate and late effect of cryotherapy on the dominant ankle joint on static balance and To determine the difference in static balance changes between both sexes.
Our result revealed that the females have significant difference in static balance than male when measured before application of cold gel pack to ankle dominant extremity with p value of overall stability index = 0.033 , p value of A/P stability index=0.043 and not for ML stability index with p value of =0.072.
Our result revealed that after using cold gel pack to ankle dominant extremity for 15 minutes has no statistically significant difference on all aspect of static balance in female group. In over stability index there was no statistically significant difference after assessment immediately, after 30 minutes and after 60 minutes with p value =0.66. In over A/P stability index there was no statistically significant difference after assessment immediately, after 30 minutes and after 60 minutes with p value =0.196. and In over M/L stability index there was no statistically significant difference after assessment immediately, after 30 minutes and after 60 minutes with p value =0.989.
Also the result revealed that after using cold gel pack to ankle dominant extremity for 15 minutes has no statistically significant difference on all aspect of static balance in males group. In over stability index there was no statistically significant difference after assessment immediately, after 30 minutes and after 60 minutes with p value =0.382, In over A/P stability index there was no statistically significant difference after assessment immediately, after 30 minutes and after 60 minutes with p value =0.525 and In over M/L stability index there was no statistically significant difference after assessment immediately, after 30 minutes and after 60 minutes with p value =0.46.
In posttest the difference between female and male in over stability index shows insignificantly difference immediately posttest with p value 0.063, insignificantly difference 30 minutes posttest with p value 0.23 and insignificantly difference 60 minutes posttest with p value 0.682.
In A/P stability index shows insignificantly difference immediately posttest with p value 0.1, insignificantly difference 30 minutes posttest with p value 0.096 and insignificantly difference 60 minutes posttest with p value 0.363.
In M/L stability index shows no significantly difference immediately posttest with p value 0.068, insignificantly difference 30 minutes posttest with p value 0.518 and insignificantly difference 60 minutes posttest with p value 0.729.
So the application of cold gel pack to ankle dominant extremity for 15 minutes has no effect on all aspect of static balance and this result may be due to that when temperature of nerve decrease, conduction velocity of nerve declines in proportion to the duration and degree of the temperature change.it is not identical at the fibers which different in diameters; rather investigates indicate cold has the highest effect on conduction by myelinated and small fibers and the smallest effect on conduction by unmylinated and large fibers.
A small diameter-mylinated and pain transmitting A-delta fibers demonstrate the highest reduction in conduction velocity in response to the cooling [26].but afferent fibers that translate the proprioceptive information from muscle spindle to the central nervous system are type of I Alfa and II meaning large myelinated fiber that have fast conduction [27].so it is possible that is less affect by cold
These findings were consistent with previous studies. Douglas et al., 2013 found that there was no statistically significant difference in static balance after 15 minutes ice water immersion to ankle joint [22], also Williams et al., 2013 found that there was no statistically significant difference in static balance after 20 minutes crushed ice bag to the ankle joint [28], Costello and Donnelly, 2011 found that that there was no statistically significant difference in static balance after 30 minutes water immersion to the knee [29].
Immersion of the ankle joint in cold water at a temperature of 4-°C for five, fifteen, and twenty minutes did not significantly affect the joint position sense of the ankle joint [30,31]. Immersion of the foot and ankle joint in cold water (1°C) did not disturb sensory perception [32].Cold water immersion thirty minutes duration to the subject’s umbilicus level did not significantly change the weight-bearing or non-weight-bearing assessment of knee joint position sense [29].The same results arisen from an investigation of the shoulder joint after the application of a cubed ice compress for thirty minutes [33].
These findings were contradicted with previous studies. Oliveira et al., 2010 found that there was statistically significant difference in knee position sense after 20 minutes crushed ice bag application to knee joint [34], also Surenkok et al., 2008 found that there was statistically significant difference in balance after 30 minutes cold pack to the knee joint [35], Wassinger et al., 2007 found that that there was statistically significant difference in static balance after 20 minutes ice bag to the shoulder extremity [36].all the previous studies maintain that application of cryotherapy locally impairs deep feeling in the body, and they totally conclude that neuromuscular deficits occur after cryotherapy application and instruct athletes against taking dynamic training immediately after cryotherapy.
Limitation:
All subjects joining in this study had uninjured ankels.Since the subjects injury may affect results of the current study.
Conclusion:
The result of current study suggest that 15 minutes of cold gel pack on ankle dominant extremity have no effect on static balance on both male .
Implementations:
The findings of the current study could be implemented in the following ways:
- Decision making concerning the use of cryotherapy within a treatment sitting or when considering return to activity after an athletic injury.
Recommendations:
The results of this study considered the following recommendations:
- Future investigates are recommended to study the effect of different cryotherapy application on static and dynamic balance.
- Future investigates are recommended to study the effect of cryotherapy on different joint in static and dynamic balance.
- Future investigates are recommended to study the effect of cryotherapy on static and dynamic balance in injured subject.
- Future investigates are recommended to study the effect of cryotherapy on static and dynamic balance in athletic subject.
Abbreviations:
OSI: Overall Stability Index.
APSI: Anterior/Posterior stability Index.
MLSI: Medial/Lateral stability Index.
T-Statistic: Un-Paired T-Test
p-value: Probability value.
* S: Significant
Pre: Pre-treatment
Post: Post-treatment.
SD: Standard Deviation.
MD: Mean Difference.
% of impr: Percentage of improvement.
F-statistics: ANOVA test
Acknowledgements
The authors express their thankful to all subjects who participated in the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Reference:
- Zagrobelny Z. & Zimmer, K. The use of cryogenic temperatures in sports medicine and physiotherapy. Rehabilitacja Medyczna .1999; Vol. 94, No. 15: 8 – 13
- Jezierski, C. Methodology and principles of local cryostimulation techniques. Acta Bio – Optica et Informatica Medica. 2006; Vol. 3, No.12: 200 – 201
- Kennet J, Hardaker N, Hobbs S, et al. Cooling efficiency of 4 common cryotherapeutic agents. J Athl Train. 2007;42:343-8.
- Kanlayanaphotporn R, Janwantanakul P. Comparison of skin surface temperature during the application of various cryotherapy modalities. Arch Phys Med Rehabil.2005;86:1411-15.
- Cina-Tschumi B. Evidence-based impact of cryotherapy on postoperative pain, swelling, drainage and tolerance after orthopedic surgery]. Pflege .2007;20:258-67.
- Algafly AA, George KP. The effect of cryotherapy on nerve conduction velocity, pain threshold and pain tolerance. Br J Sports Med. 2007;41:365-9.
- Bleakley C, McDonough S, MacAuley D. Use of ice in the treatment of acute soft-tissue injury: a systematic review of randomized controlled trials. Am J Sports Med. 2004;32:251-261.
- Tee JC, Bosch AN, Lambert MI. Metabolic consequences of exercise-induced muscle damage. Sports Med 2007; 37:827-836.
- Bleakley CM, Costello JT, Glasgow PD.Should Athletes Return to Sport After Applying Ice? Sports Med . 2012.;42(1):69-87 .
- Ruiz DH, MyrerJW, Durrant E, FellinghamGW. Cryotherapy and sequential exercise bouts following cryotherapy on concentric and eccentric strength in the quadriceps. J AthlTrain. 1993;28(4):320.
- Pereira LG, Pereira R, Neto OP, Magini M. The short and long term effects of tibialis anterior local cooling on dorsiflexion force. J Human Kinet. 2010 ;26(â€1):65-71
- Schultz AB, Alexander NB & Ashton-Miller JA .Biomechanical analyses of rising from a chair. Journal of Biomechanics. 1992; 25: 1381-1391.
- 2. Berg K, Wood-Dauphinée S, Williams JI & Gayton D .Measuring balance in the elderly: preliminary development of an instrument. Physiotherapy Canada. 1989; 41: 304-311.
- Hrysomallis C. Relationship between balance ability, training, and sports injury risk. Sport Med .2007; 37:547-556.
- Salavati M, Moghadam M, Ebrahimi I Arab AM. Changes in postural stability with fatigue of lower extremity frontal and sagittal plane movers. Gait Posture. 2007; 26:214-218
- Clark B, Manini T, Thé D, Doldo N, Ploutz-Snyder L. Gender differences in skeletal muscle fatigability are related to contraction type and EMG spectral compression. J Appl Physiol .2003; 94:2263-2272
- Hirabayashi SIY. Developmental perspective of sensory organization on postural control. Brain Dev. 1995; 2:111-113.
- Kellis E, Kouvelioti V. Agonist versus antagonist muscle fatigue effects on thigh muscle activity and vertical ground reaction during drop landing. J Electromyogr Kinesiol. 2009; 19:55-64
- Richendollar ML, Darby LA, Brown TM. Ice bag application, active warm-up, and 3 measures of maximal functional performance. J Athl Train. 2006;41(4):364.
- Ingersoll CD, Knight KL, Merrick MA. Sensory perception of the foot and ankle following therapeutic applications of heat and cold. J Athl Train.1992;27(3):231.
- Arnold BL, Schmitz RJ. Examination of balance measures produced by the Biodex Stability System. J Athl Train.1998 ;33(4):323.
- Douglas, Matthew, et al. “Immediate effects of cryotherapy on static and dynamic balance.” International journal of sports physical therapy 8.1 9;2013.
- Pereira HM, Campos TF, Santos MB, Cardoso JR, Garcia M, Cohen M. Influence of knee position on the postural stability index registered by the Biodex Stability System. Gait Posture .2008; 28:668-672.
- Duecker, Jody. Measurement of Validity for Balance Assessments using a Modified CTSIB Sway Index Versus a Biodex Sway Index. Diss. The University of Akron.;2013.
- Paddon-Jones, D. J., & Quigley, B. M. Effects of cryotherapy on muscle soreness and strength following eccentric exercise. The International Journal of Sports Medicine. 1997;18 (8),:588-593.
- De Jesus PV,Hausmanowa-petrusewicz I,Barchi RL.The effect of cold on nerve conduction of human slow and fast nerve fibers.Neurology. 1973;23:1182-9.
- Cameron MH.Pysical Agents in Rehabilitation:From Research to Practice .Philadelphia:WB Saunders.2003;P:140.
- E.E. Williams, S. J. Miller, W. J. Sebastianelli, and G. L. Vairo.”Comparative immediate functional outcomes among cryotherapeutic interventions at the ankle,” International Journal of Sports Physical Therapy. 2013; vol. 8, no. 6:828-837.
- J. T. Costello and A. E. Donnelly, Effects of cold water immersion on knee joint position sense in healthy volunteers,” Journal of Sports Sciences.2011; vol. 29, no. 5 :449-456.
- J. LaRiviere and L. R. Osternig. “The effect of ice immersion on joint position sense,” Journal of Sport Rehabilitation.1994; vol. 3, no. 1: 58-67.
- R. Khanmohammadi, M. Someh, and F. Ghafarinejad.”The effect of cryotherapy on the normal ankle joint position sense,” Asian Journal of Sports Medicine.2011;vol. 2, no. 2: 91-98,.
- C. D. Ingersoll, K. L. Knight, and M. A. Merrick. “Sensory perception of the foot and ankle following therapeutic applications of heat and cold,” Journal of Athletic Training. 1992;vol. 27, no. 3:231-233.
- G. C. Dover and M. E. Powers. “Cryotherapy does not impair shoulder joint position sense,” Archives of Physical Medicine and Rehabilitation. 2004; vol. 85, no. 8:1241-1246.
- R. Oliveira, F. Ribeiro, and J. Oliveira.”Cryotherapy impairs knee joint position sense,” International Journal of Sports Medicine. 2010; vol. 31, no. 3: 198-201.
- O. Surenkok, A. Aytar, E. H. Tüzün, and M. N. Akman. “Cryotherapy impairs knee joint position sense and balance,” Isokinetics and Exercise Science. 2008; vol. 16, no. 1:69-73.
- C. A. Wassinger, J. B. Myers, J. M. Gatti, K. M. Conley, and S. M. Lephart.”Proprioception and throwing accuracy in the dominant shoulder after cryotherapy,” Journal of Athletic Training.2007.;vol. 42, no. 1:84-89.